In osteopathy, we pay a lot of attention to the 3 anatomical links between all the components of the human body: the fascial link, the vascular link and the neurological one. These 3 links have their own anatomical substrate but, in a global vision, it is the connective tissue, through its fascial network and its extracellular matrix that connects these 3 links[1].
In acupuncture, the concept of energy is essential and it could also, more or less, be in certain schools of osteopathy. But how can we understand, approach and evaluate the energy in a truly osteopathic way?
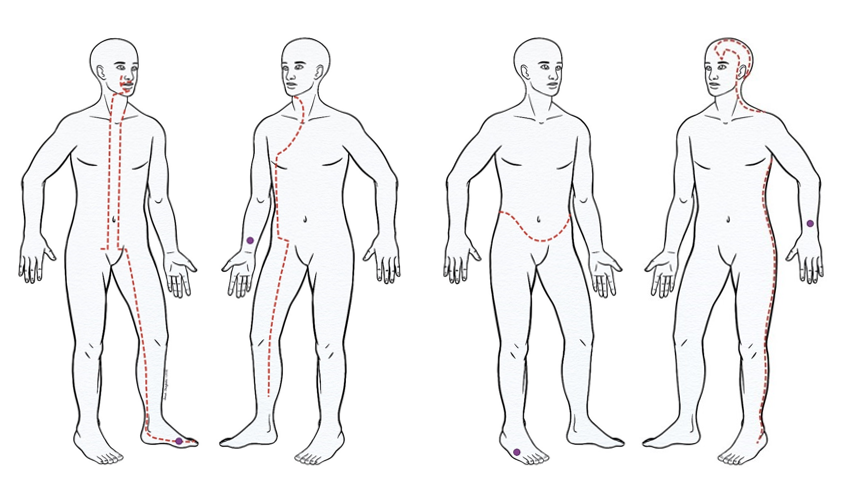
“The wind blows, the leaf moves “. By not objectively paying attention to the structure (the leaf), I will not see, I will not grasp the energy (the wind). Then again, the structure is needed in order to “materialize” and perceive the energy. We can therefore concede that connective tissue, present throughout and filling everything, renders this invisible energy, which animates all living beings, palpable through its suppleness and its elasticity. With this in mind, we have, for many years, systematically integrated the tissular reality of the meridians and the acupuncture points in our osteopathic practice, in the same way as all other physical structures. Following on from our previous publications[2], the Extraordinary Vessels (EOV)[3] described in acupuncture and their master points[4] have become nowadays a new source of inspiration.
After an Osteopathic Mechanical Link seminar, Dr René Descartes, co-writer for this paper, shared his personal findings on the Extraordinary Vessels (EOV) suggesting some reconciliation between the 8 EOV and the 8 units of Osteopathic Mechanical Link[5].
Would each of those EOV represent a particular functional or anatomical unit?
Is the EOV model really interesting to take into consideration for the osteopath?
If the master points can easily be tested, is it possible to determine which unit or units are of priority for treatment?
We could also consider that stimulating master pts and/or others key points of the EOV may consolidate and amplify the treatment of a unit!?
It has been demonstrated in practice that the key points of the EOV are often found to present tissular fixations linked to the patient’s symptoms. Furthermore, treatment of these osteopathic lesions yielded surprising responses, even with complex, chronic or recurring, pathologies for which we had limited results.
Experience and clinical results have confirmed the pertinence of this approach. We are nowadays convinced that the EOV system fully deserves to be integrated as an extra diagnostic and treatment tool in osteopathy.
[1] Helene M. Langevin, David L. Churchill, Marilyn Cipolla, Mechanical signaling through connective tissue: a mechanism for the therapeutic effect of acupuncture, 2001
It is possible to define the osteopathic lesion as a scar that can affect all tissues of mesodermic origins: bones, joints, muscles, tendons, ligaments, fascias, aponeuroses, dermis, vascular sheaths, etc.
Even if the nervous system is derived from the ectoderm, we should keep in mind that more than 50% of the peripheral nerves are connective tissue originating from the mesoderm (epineurium, perineurium, endoneurium ) in addition to the connective sheaths (paraneurium) surrounding the nerves along their path.
[2] Chauffour P., Prat E., Michaud J., LMO Points clés du système nerveux périphérique, Editions Sully, 2017.
[3] Also known as extraordinary meridians.
[4] Appelés aussi points de commande ou points maître.
[5] Cf. Diagnostic and treatment chapter using the Osteopathic Mechanical Link methodology.