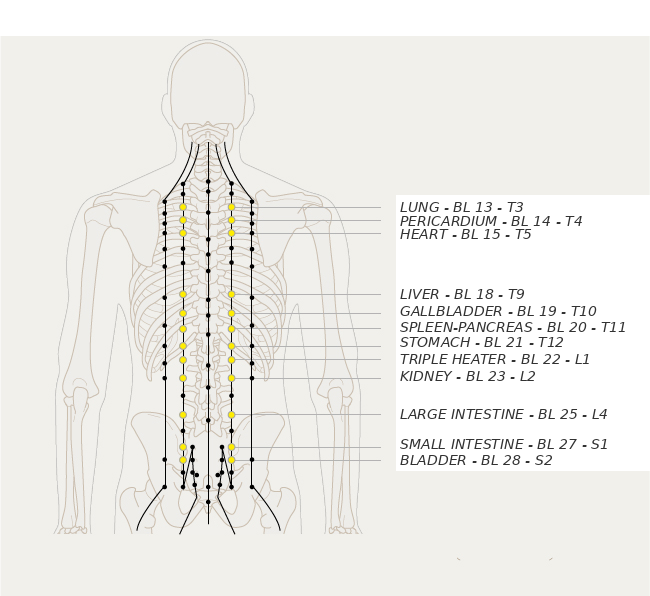
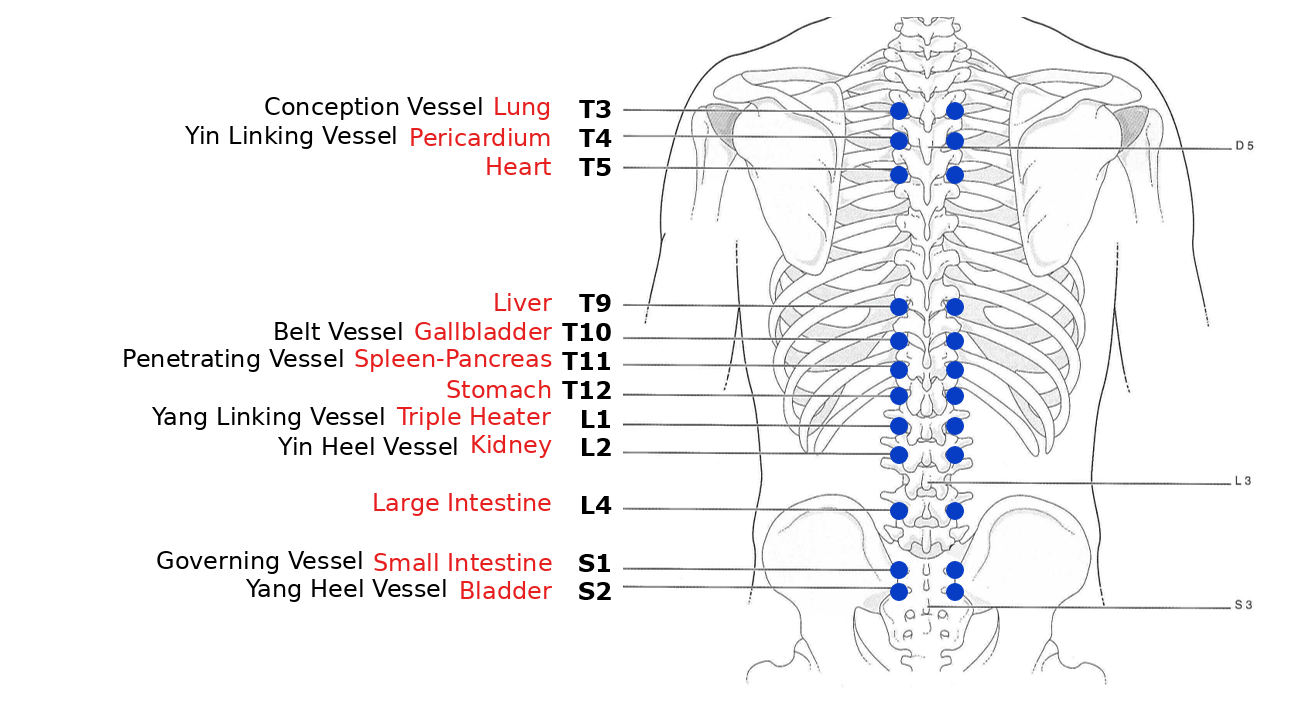
It is well known that the vertebral keyboard, via the sympathetic trunk, has a major influence on organ function.
This is a two-way segmental relationship: a vertebral articular fixation can affect an organ (somatovisceral reflex) and, conversely, a visceral dysfunction can be reflected at the corresponding spinal level (viscerosomatic reflex).
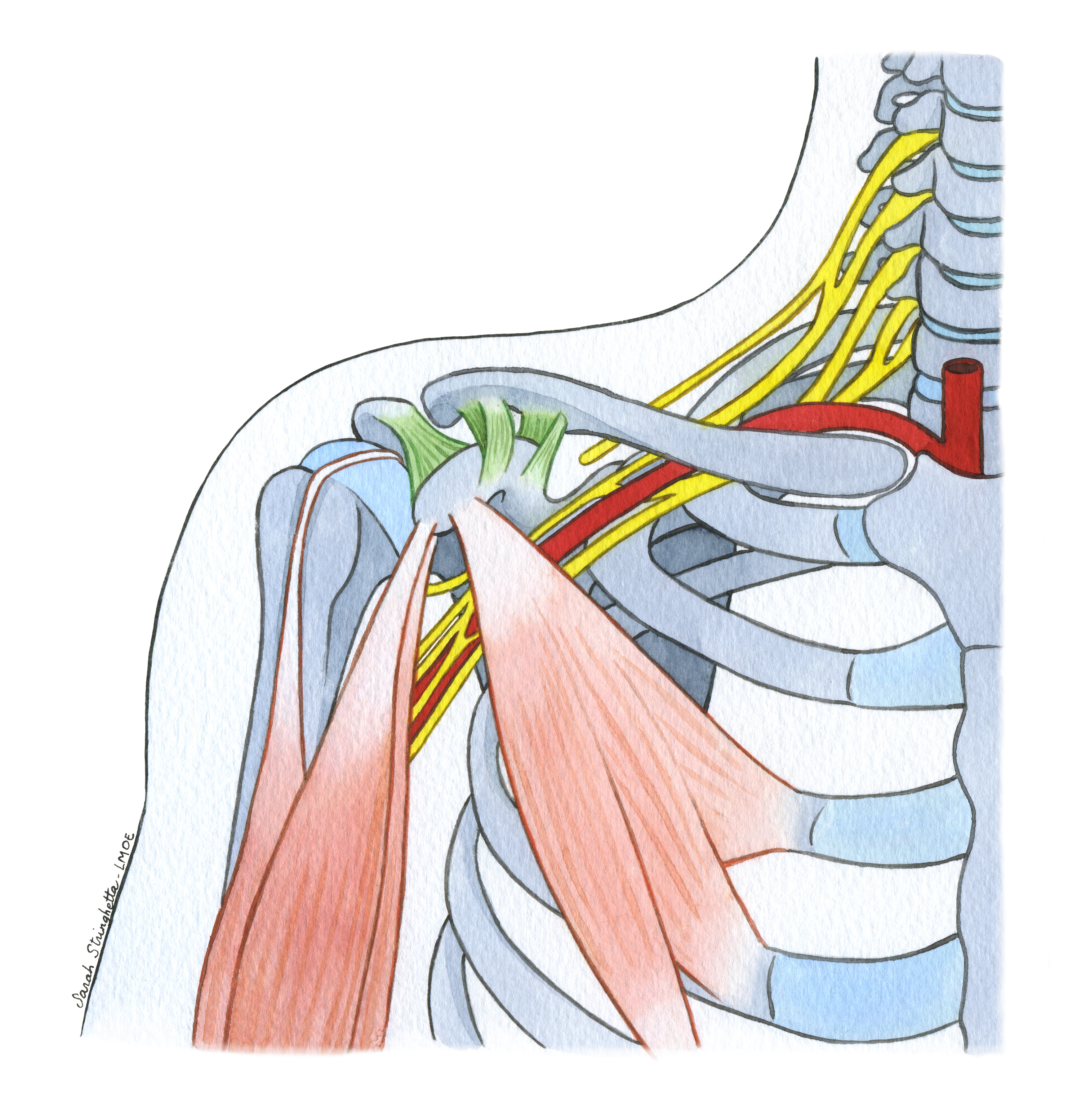
In a segmental framework, these correlations form a complex network. Each node can communicate with any other: dermatome, myotome, sclerotome, viscérotome. It is classically described, according to Head[1], that a disorder of the gallbladder may be associated with muscular manifestations in the shoulder.
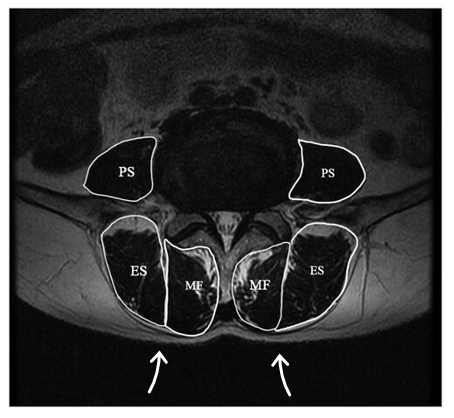
But this can also involve the skin (dermatome) or bony structures (sclerotome) corresponding to the same segmental level.[2]
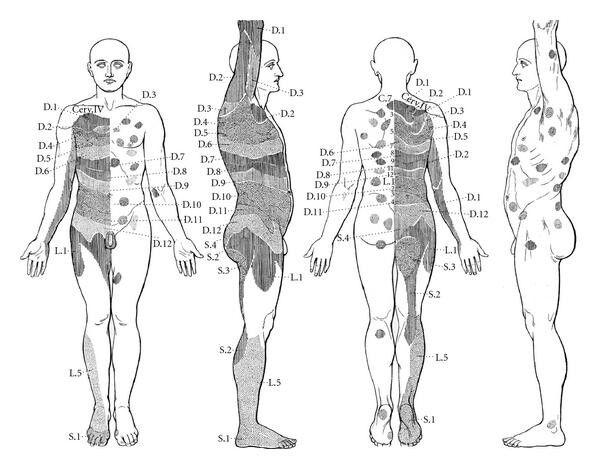
[1]In the 1890s, the neurologist Sir Henry Head identified certain skin zones that develop sensitivity (allodynia) during visceral pathology (Head’s zones). He also highlighted the existence of specific points within these zones, which he called “maximum points.”
[2]Wancura-Kampik, I. (2012). Segmental anatomy: The key to mastering acupuncture, neural therapy, and manual therapy (1st ed.). Elsevier Urban & Fischer.